
AMD (Age-related macular degeneration)
Age-related macular degeneration (AMD) is the third most common eye disease after cataract and glaucoma, accounting for almost 10% of all eye diseases. This disease of the retinal center includes the sensory cells of the retina (photoreceptors), the pigment epithelium, Bruch’s membrane and the underlying choroid.
-
GENERAL, EXPLANATION OF TERMS
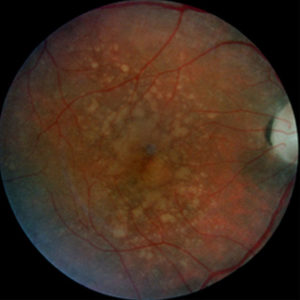 Dry macular degeneration with large, confluent drusen and pigment irregularity.
Dry macular degeneration with large, confluent drusen and pigment irregularity.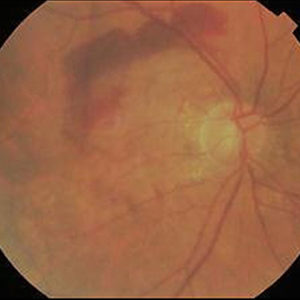 Wet age-related macular degeneration with hard exudates and bleeding.
Wet age-related macular degeneration with hard exudates and bleeding.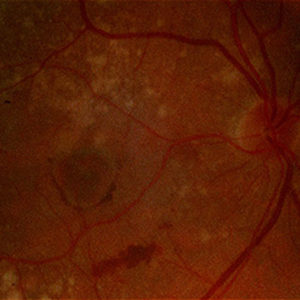 Transition of a dry into a wet macular degeneration.
Transition of a dry into a wet macular degeneration.Macula means spot. But the macula is also referred to as the so-called yellow spot or the point of sharpest vision. It is also referred to as the center of the retina, without whose functioning the fixation and recognition of objects, i.e. reading, writing, recognition of faces, watching television etc. is not possible. This region of the retina is affected by AMD. The impairment of sharp vision does not affect the peripheral field of vision. I.e. seeing at a distance, activities such as working in the household or garden are hardly impaired. Even in severe cases, the risk of helplessness or blindness is rare, however the ability to drive, for example, can be lost.
From the age of 60, rarely before, the ophthalmologist can observe corresponding changes long before the first clinical symptoms appear. With increasing age, the risk of developing AMD with the consequence of a deterioration of vision increases continuously. Genetic factors influence the individual risk, i.e. also the time of occurrence of AMD. However, probably everyone would develop AMD if they were old enough. It is the most common cause of severe visual impairment in old age and affects about 25% of people over the age of 65.
There are 2 forms of AMD: Dry AMD – which accounts for 85 to 90% of cases – leads to a slow, gradual deterioration in visual function over the course of several years to decades. There is no therapy for this form. In 10 to 15% of patients, it eventually turns into wet AMD. This is more aggressive and leads to a rapid deterioration of vision. Only 10% of the cases with severe visual impairment are caused by the dry form, and 90% by wet AMD, which, if left untreated, can lead to complete loss of central vision.
One might wonder why this disease affects the center of the retina and no other areas of the retina. The high susceptibility results from the anatomy of the retinal center, which is specialized for maximum visual acuity performance. In order to achieve this, blood vessels in the macula that would impair optimal vision have been omitted. Thus, the nutrition and oxygen supply of this area is only indirectly provided by the pigment epithelium (visual pigment) and the choroid, which are located behind the retina. This means that all supply routes are long and susceptible to age-related and pathological changes, especially deposits that lead to diffusion barriers.
Many biochemical metabolic processes are associated with high visual performance. Their waste products can be easily removed at a young age. With increasing age, however, the disposal capacity decreases. Waste products consequently remain under the retina and the so-called Bruch’s membrane. With this, a layer behind the pigment epithelium between the retina and the choroid, thickens. This barrier reduces the supply and disposal of nutrient and waste products to and from the macula.
-
CAUSES
Clinically, the ophthalmologist then sees yellow spots on the back of the eye, which are called drusen. Isolated small drusen are found in many people over 50 years of age. The more and larger the drusen become, the greater the risk that they will lead to a disturbance of the light-sensing cells in the center of the retina. At this stage, however, patients do not notice anything. Together with further changes in the cells of the pigment epithelium, this condition can progress to AMD. As long as the function is not disturbed, it is called maculopathy. The changes remain unnoticed by the patient, and treatment is not necessary nor possible. Only when the changes lead to a decrease in visual acuity, initially mainly to poorer contrast and darkness vision, and later to problems with reading, is it called AMD.
The exact cause of AMD is not known. Besides age, various risk factors have been found. These include a genetic disposition (parents and/or siblings also have AMD), smoking (also ex-smokers), lipid metabolism disorders (hypercholesterolemia), malnutrition and obesity. As well as, diseases of the cardiovascular system, light iris and heavy (unprotected) exposure to sunlight over the course of life. Women are more frequently affected than men. Of course, one eye is also at high risk if the other eye is already diseased.
As already mentioned, a distinction between a dry or non-exudative and a wet or exudative form is crucial for therapeutic options. The dry or non-exudative form is characterized by a reduction to atrophy of the pigment epithelium, the fine choroidal vessels (choriocapillaris) and the sensory cells of the retina. There is no established treatment option for this form so far.
In the exudative or wet form, in addition to the changes known from the dry form, newly formed blood vessels (neovascularization) are found as a result of the local nutritional disturbance and the impaired oxygen supply. These newly formed vessels are an attempt by the undersupplied retina to compensate for the oxygen deficiency caused by the barriers. This problem is only present at the center of the retina and has nothing to do with nutrition in general. The new vessels are less dense and stable than the retina’s natural vessels, allowing blood components to leak into the retina.
-
SYMPTOMS
As a result of the accumulation of fluid (edema) in the retina, distorted, blurred nebula vision occurs. In the long term, the leakage of blood components leads to scarring of the center of the retina, these areas of the retina are then blind. Those affected often recognize them on a light background as dark spots with distorted vision next to them.
-
DIAGNOSTICS
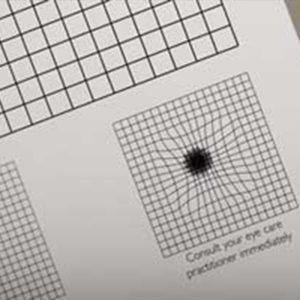 The Amsler test provides information about the patient's distorted vision.
The Amsler test provides information about the patient's distorted vision.An increased release of vascular endothelial growth factors (VEGF) was found to be the trigger for neovascularization. The neutralization of VEGF with specific so-called angiogenesis inhibitors leads to the sealing or even regression of the newly ingrown vessels. In the meantime, various drugs are available (Lucentis®, Eylea®, Beovu® and Vabysmo®), which have revolutionized the treatment of wet AMD. This not only makes it possible to prevent a loss of visual acuity, but in many cases, what was previously considered unthinkable can even maintain reading ability and improve vision over many years, although in most cases normal vision is not achieved. In addition to the above-mentioned drugs, bevacizumab, a cancer drug (Avastin ®), is used in many places as a cheaper alternative. In the short term (over 2 years) this therapy shows almost as good results as the two approved drugs, but the long-term stability and safety with regard to side effects do not speak in favor of this therapy in most cases. Beovu® has only been approved in Switzerland since 2020. Its advantage compared to already available drugs lies in a possible prolonged duration of action and thus in a reduction of the injection frequency. However, there is also an increased risk of potentially serious ocular inflammation, which is why this drug is currently only used in individual cases.
The most important criterion for the success of the treatment is the earliest possible diagnosis. And early diagnosis is also a challenge for family doctors. With the ophthalmoscope they can already make a suspected diagnosis if they see yellow spots (drusen or protein deposits) or bleeding. If there is also a distortion of the grid lines in the Amsler net, there is a suspicion of a wet macular degeneration. In this case the ophthalmologist should quickly (within days to weeks) examine the ocular fundus (ophthalmoscopy). If there is a swelling of the retina with bleeding and protein deposits in the retina, the diagnosis of a wet macular degeneration is almost certain. A fluorescein angiography (dye examination of the retinal vessels for leaks and new blood vessel formation) can then be performed. This will help to clarify the diagnosis and to assess the success of treatment in cases of questionable wet macular degeneration and to evaluate the localization and extension of new blood vessel formation under the retina. Alternatively, or complementary to fluorescence angiography, a so-called OCT angiography can be used for three-dimensional imaging of the vascular structures of the retina and the underlying choroid. This technique has the great advantage of being non-invasive.
-
TREATMENT
As soon as the diagnosis is clear, medication injections are first made into the vitreous body of the affected eye at monthly intervals. Using the so-called OCT (Optical Coherence Tomogram), assessment of the regression of fluid in the retina can be made and thus the possible need for further injections can be ascertained. As a rule, a minimum of 6 to 8 and a maximum of 10 to 12 injections are required in the first year; this, in order to achieve an optimal visual acuity result.
Two large studies (MARINA and ANCHOR study) have shown that monthly injections into the eye have few side effects and are well tolerated when administered under sterile conditions. On average, this aggressive treatment regimen achieves a visual acuity gain of two lines, which in many cases even means a largely unrestricted visual function with preservation of driving ability / reading ability.
If, on the other hand, instead of monthly – and regardless of the clinical picture – injections are applied based on the observation of a recurrence of the disease (clinically or by OCT). Or if the treatment intervals are inflexible and too long, this means fewer (5 to 6) injections, but also a lower visual acuity gain; as shown in three other studies (PIER, SUSTAIN, EXCITE).
The monthly injection causes enormous logistical problems for patients and their relatives, as well as the doctors caring for them. The compromise solution “as much gain as possible and as few injections as possible”, as investigated in the latter studies, has now become accepted in everyday clinical practice. In the past, patients were examined on a monthly basis to keep the risk of unnoticed reactivation and vision deterioration low and, if necessary, to be able to treat them early on. Nevertheless, this approach remains a compromise between optimal visual acuity results and the least possible stress for the patients. Since the monthly injection of medication into the eye is both stressful and very expensive for patients, preventive treatment is increasingly being used to keep the disease inactive, thus prevent it from worsening. The treatment intervals are gradually extended as long as the macular degeneration remains dry (no fluid is stored in the retina).
-
GENERAL PROBLEMS AND COMPLICATIONS
In principle, the progression of both wet and dry AMD cannot be prevented or reversed in the long term (i.e. over many years). However, the elimination of the risk factors that can be influenced (e.g. smoking) and possibly a vitamin-rich diet may be able to delay the progression. The combination of certain antioxidants (especially lutein) and dietary supplements (especially zinc) may be able to delay transition from a dry to a moist form in some cases. This, as shown in the much-cited ARED study, although the side effects of long-term treatment are still unclear. Various preparations are now on the market, with Ocuvite ® Lutein, and Vitalux®Plus having the largest market share. Ginkgo biloba extracts and blueberry extracts are also mentioned as a treatment for macular degeneration, but probably have no scientifically proven effect that would justify their use and the associated costs. They should therefore not be recommended. A deterioration of visual acuity in dry AMD cannot be prevented in the long term. In wet AMD, early diagnosis and therapy is the key to long-term stabilization of function.